
Diagnosing Infertility in Las Vegas: Getting the Answers You Need
Your family-building journey begins with clear answers. If you’ve been trying to conceive without success, understanding why is the most important first step — and it’s exactly where we start.
At The Fertility Center of Las Vegas, our team of reproductive endocrinologists evaluates both female and male fertility together, from the very beginning. We use a thorough, evidence-based approach to identify what’s standing between you and building the family you have always dreamed of, so we can build a treatment plan that’s truly personalized to you.
When Should You Get a Fertility Evaluation?
Fertility experts recommend seeking an evaluation in the following situations:
- Women under 35: after 12 months of trying to get pregnant without success.
- Women 35 or older: after 6 months of trying to conceive without success. Ovarian reserve declines more quickly after 35, so earlier testing means more options.
- Pre-existing conditions: if you have conditions that can affect fertility — such as polycystic ovary syndrome (PCOS), endometriosis, recurrent miscarriages, or male fertility concerns — an earlier evaluation is recommended, regardless of how long you’ve been trying.
Not sure whether now is the right time? Our team is here to help you figure that out. A brief conversation with one of our Las Vegas specialists can give you a clear sense of whether testing makes sense for you right now — and what to expect if it does.
Female Infertility Diagnosis
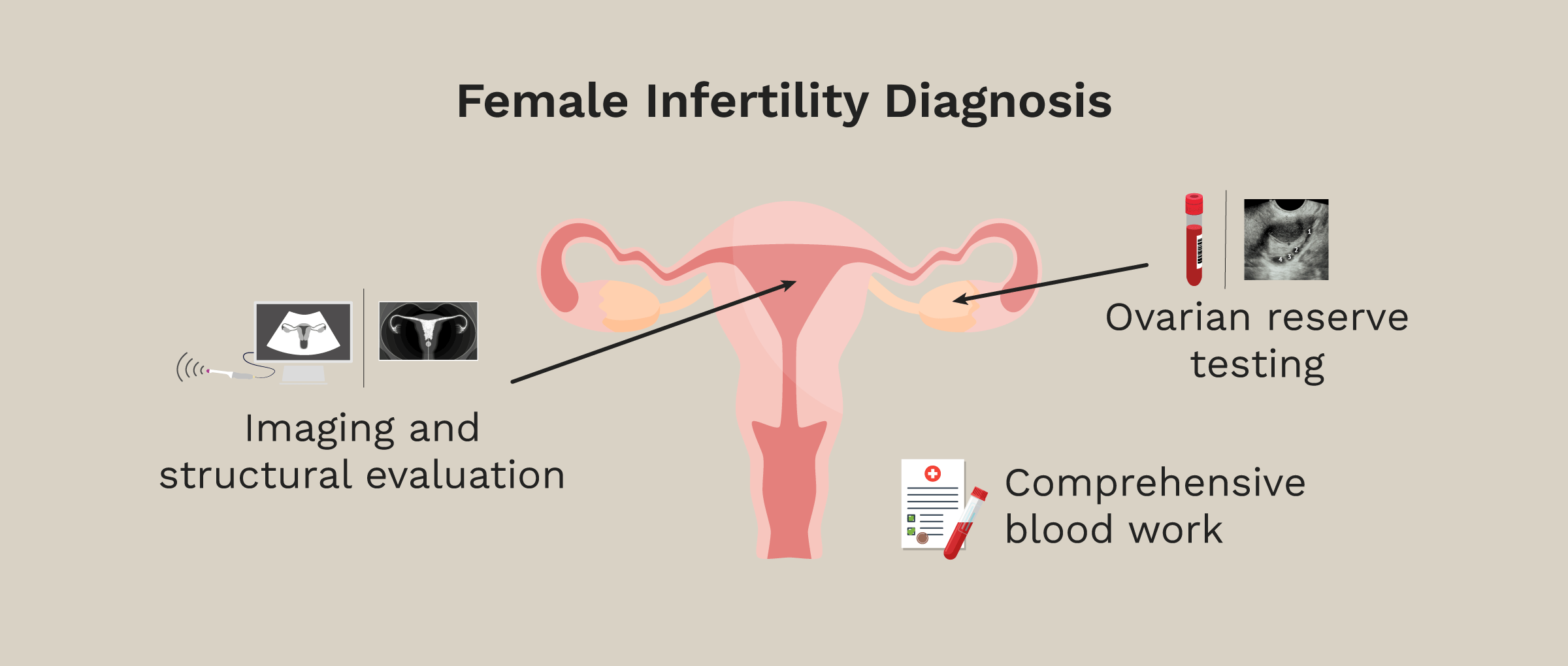
Female fertility evaluation at The Fertility Center of Las Vegas focuses on three key areas: the ovaries, fallopian tubes, and uterus.
These tests help us understand ovulation, egg supply, and whether the reproductive organs are functioning properly. Our goal is to identify any structural abnormalities or hormonal problems that may prevent ovulation, fertilization, or embryo implantation.
The primary fertility tests for women include:
- Ovarian reserve testing: AMH (Anti-Müllerian Hormone), cycle day 3 hormone levels (FSH, LH, estradiol), and an antral follicle count (AFC) via transvaginal ultrasound.
- Comprehensive blood work: A blood draw to assess additional hormones and markers that can affect fertility and overall reproductive health.
- Imaging and structural evaluation: Transvaginal ultrasound for general structural assessment of the uterus and ovaries, sonohysterogram (SHG) for uterine evaluation, and tubal patency testing (HyFoSy, HyCoSy, or HSG).
For a detailed look at each of these tests, visit our Fertility Tests for Women page.
Male Infertility Diagnosis
In approximately 40–50% of infertility cases, a male factor is involved. This is why we evaluate both partners from the very beginning — so nothing gets missed and no time is lost.
The primary fertility test for men at our Las Vegas clinic is a comprehensive semen analysis, which evaluates sperm concentration, morphology (shape), and motility (movement). Depending on your initial results and medical history, additional testing may include:
- Male hormone evaluation: assesses testosterone and other hormones that influence sperm production.
- Sperm DNA fragmentation testing: evaluates the integrity of the genetic material within the sperm, which can affect fertilization and embryo development.
- Path Sperm QT: assesses sperm quality and function by examining epigenetic factors.
- Semen culture: performed to rule out infections that could affect sperm health or fertility.
For a complete overview of male fertility testing, visit our Fertility Tests for Men page.
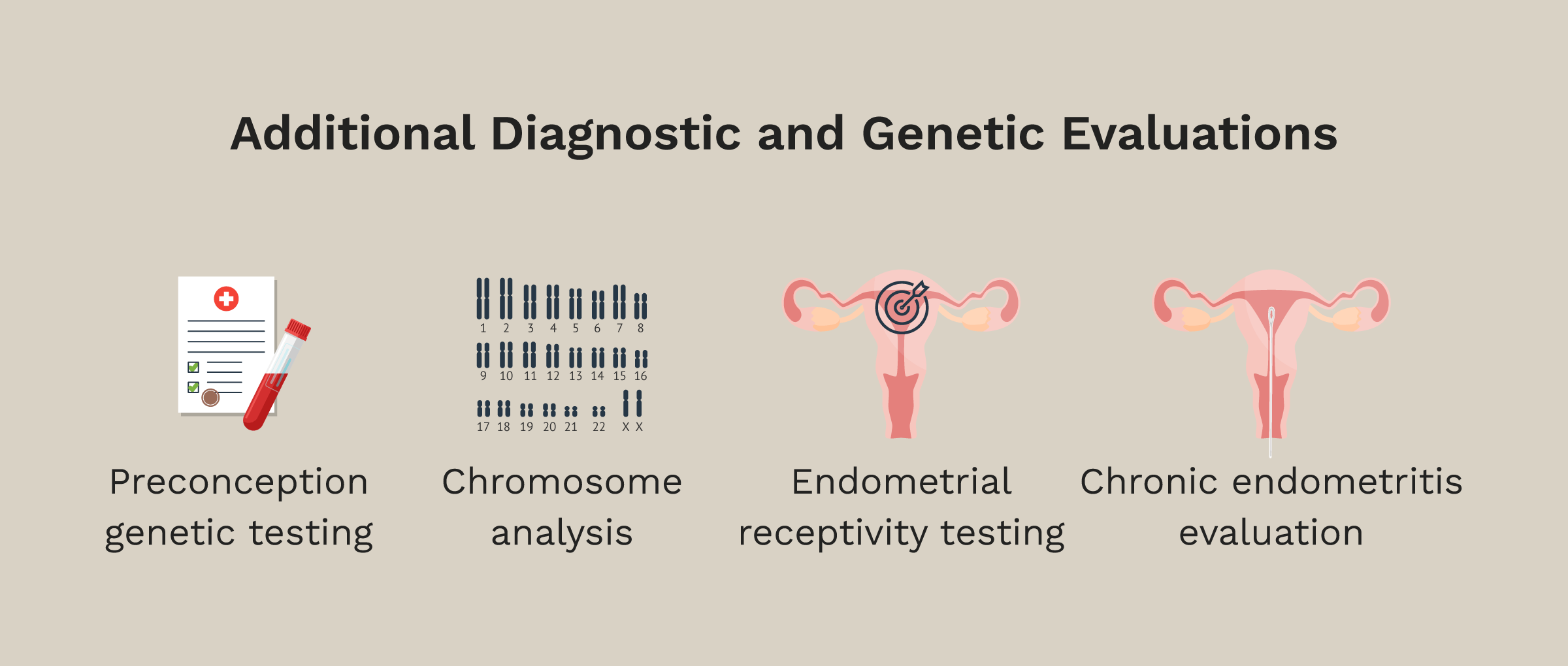
Additional Diagnostic and Genetic Evaluations
At The Fertility Center of Las Vegas, we go beyond the standard work-up to make sure you have the most complete picture possible before starting treatment. Some of these evaluations are recommended for all patients; others are added based on your specific history and circumstances.
- Preconception genetic testing (carrier screening): a simple saliva or blood test recommended for all patients that checks whether you or your partner carry genes for certain inherited conditions.
- Chromosome analysis (karyotyping): a blood test that examines the number and structure of chromosomes in you or your partner’s cells. Recommended when there is a history of recurrent miscarriages, previous implantation failures, or a known or suspected chromosomal condition.
- Endometrial receptivity testing (ReceptivaDx): a uterine biopsy test that detects uterine inflammation caused by silent endometriosis – a common but often overlooked cause of implantation failure.
- Chronic endometritis evaluation: assesses for low-grade uterine inflammation that can interfere with implantation, recommended when there is a history of failed transfers or recurrent loss.
Together, these evaluations allow us to personalize your care and give every embryo transfer the best possible chance of success.
From Diagnosis to Treatment: Your Next Steps
Once your diagnostic work-up is complete, our specialists will explain all findings during a results consultation. A diagnosis isn’t an ending — it’s the starting point for choosing the right treatment plan for you. Depending on what we find, your options may include:
- Ovulation induction: medications to stimulate ovulation for patients who are not ovulating regularly.
- Intrauterine Insemination (IUI) or Intratubal Insemination (ITI): for cases of mild male factor infertility, cervical issues, or unexplained infertility. (Learn more about IUI | Learn more about ITI)
- In Vitro Fertilization (IVF): the most effective option for overcoming tubal obstructions, severe endometriosis, low ovarian reserve, or moderate-to-severe male factor infertility. (Learn more about IVF)
- Other targeted treatments: including donor egg, donor sperm, embryo donation, or gestational carrier pathways, depending on your diagnosis and goals.
Whatever your diagnosis, our commitment at The Fertility Center of Las Vegas is to walk alongside you through every step — making sure the path forward always gives you the best possible chance of building your family.
Ready to Start? Let’s Find Your Answers Together
The most important thing you can do right now is get a clear picture of where things stand. Schedule your fertility evaluation at The Fertility Center of Las Vegas — and let’s figure out your best path forward, together.







